





Keratosis Pilaris
Keratosis pilaris is a very common skin condition appearing as rough, whitish papules (small, solid bumps) on the upper arms and thighs of children and young adults especially, although older adults can also be affected. These bumps arise when a hair follicle becomes plugged with keratin, a protein found in skin, hair, and nails. The bumps are sometimes described as feeling rough, or like “goose bumps” or “chicken skin.”
When keratosis pilaris appears on the face, it can be mistaken for acne. However, acne creams will not make the keratosis pilaris better and may aggravate the bumps. A common mistake many people make is to try and scrub the bumps away, but this can make the condition worse. A medical professional can recommend creams that should improve the keratosis pilaris, and it often goes away on its own.
Who's At Risk?
Keratosis pilaris can affect people of any age, race / ethnicity, and sex. It is more common in females and in people with sensitive skin.
Keratosis pilaris often develops by age 10 and can worsen during puberty or pregnancy. However, it frequently improves or even goes away by early adulthood.
Keratosis pilaris can affect 50%-80% of teenagers and up to 40% of adults. Many people have a family history of keratosis pilaris. A large proportion of individuals with ichthyosis vulgaris (an inherited skin condition characterized by very dry, very scaly skin) also report the presence of keratosis pilaris.
Signs & Symptoms
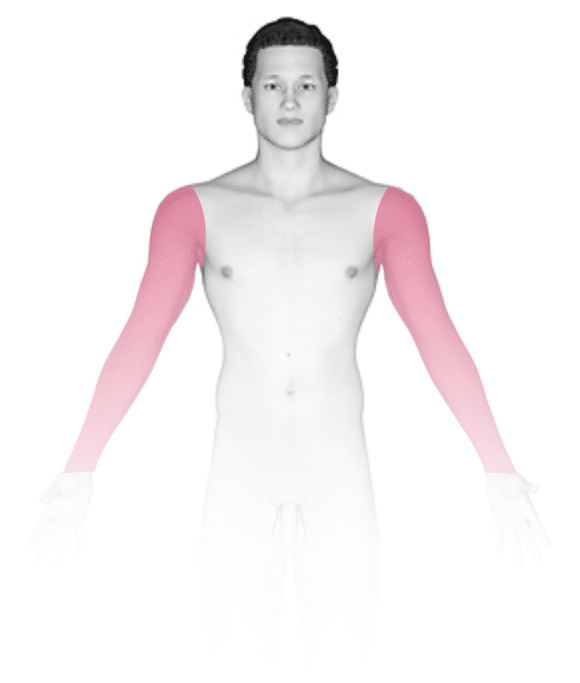
The most common locations for keratosis pilaris include:
- Back of the upper arms.
- Front of the thighs.
- Buttocks.
- Cheeks, especially in children.
Keratosis pilaris lesions are tiny (1 mm) white-to-gray bumps centered in the hair follicle. Sometimes a thin, red ring may surround the white bump, indicating inflammation. In darker skin colors, the red area around the bumps may be harder to see or may appear darker brown. The bumps all look very similar to one another, and they are evenly spaced on the skin’s surface.
Rarely, people with keratosis pilaris may experience mild itching.
Keratosis pilaris tends to improve in warmer, more humid weather, and it may worsen in colder, drier weather.
Self-Care Guidelines
There is no cure for keratosis pilaris, but its appearance can be improved. It is often helpful to keep the skin moist (hydrated) and to use mild, fragrance-free cleansers with daily applications of moisturizer.
Creams and ointments are better moisturizers than lotions, and they work best when applied just after bathing, while the skin is still moist. The following over-the-counter products may be helpful:
- Preparations containing alpha-hydroxy acids such as glycolic acid or lactic acid (eg, CeraVe SA Cream for Rough & Bumpy Skin)
- Creams containing urea (eg, Cetaphil Rough & Bumpy Daily Smoothing Moisturizer)
- Hydrocortisone (eg, Cortaid) cream 1% (if the areas are itchy)
Do not try to scrub the bumps away with a pumice stone or similar harsh exfoliant; these approaches may irritate the skin and worsen the condition. Similarly, try to avoid scratching or picking at the bumps, as these actions can lead to bacterial infections and scarring.
Treatments
Keratosis pilaris may improve with time. However, it is generally regarded as a long-lasting (chronic) skin condition. Treatments are aimed at controlling the rough bumps, not curing them. Keratosis pilaris bumps will come back if therapy is stopped.
To treat the bumps of keratosis pilaris, your medical professional may recommend a topical cream or lotion containing:
- Prescription-strength alpha- or beta-hydroxy acids (glycolic acid, lactic acid, salicylic acid).
- Prescription-strength urea (Carmol, Aluvea, Keralac).
- A retinoid such as tretinoin (Retin-A ) or tazarotene (Avage, Tazorac).
- Prescription-strength hydrocortisone cream if inflammation is present.
Visit Urgency
Keratosis pilaris is not a serious medical condition and it has no health implications. However, if self-care measures are not improving the appearance of the skin and it continues to bother you, see a dermatologist or another medical professional who may be able to prescribe stronger treatments. If pus-filled bumps appear, that indicates a secondary bacterial infection, and it is also important to seek care if this occurs.
References
Bolognia J, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia, PA: Elsevier; 2018.
James WD, Elston D, Treat JR, Rosenbach MA. Andrew’s Diseases of the Skin. 13th ed. Philadelphia, PA: Elsevier; 2019.
Kang S, Amagai M, Bruckner AL, et al. Fitzpatrick’s Dermatology. 9th ed. New York, NY: McGraw-Hill Education; 2019.
Paller A, Mancini A. Paller and Mancini: Hurwitz Clinical Pediatric Dermatology. 6th ed. St. Louis, MO: Elsevier; 2022.
Last modified on February 28th, 2023 at 8:37 pm
Not sure what to look for?
Try our new Rash and Skin Condition Finder